Restoring function,
rebuilding limbs.
Comprehensive specialist care for limb deformity, length discrepancy, bone infection and the complications of major trauma. Based in Manchester, treating patients from across the United Kingdom and beyond.

A practice built on volume, precision and pioneering technique.
Higher surgical training in the North West, fellowship at the Leeds Limb Reconstruction Unit, and dedicated experience in Tygerberg, South Africa — converging into one of the highest-volume circular frame practices in the United Kingdom.

Mr Nesbitt is a Consultant Trauma and Limb Reconstruction Surgeon based at Manchester Royal Infirmary, where he forms part of the major trauma consultant team and leads on complex reconstruction of traumatically injured limbs. His elective practice focuses on chronic bone infection, limb length discrepancy, multiplanar deformity correction, and salvage surgery for the complications of trauma.
As one of the highest-volume circular frame surgeons in the UK, he treats more than one hundred open fractures every year. He also leads the only multi-disciplinary Transverse Cortical Tibial Transport (TTT) service in the UK offering this technique for vascular ulceration and claudication pain — in partnership with the Manchester vascular team.
Beyond clinical practice, Mr Nesbitt serves as Governance Lead at Manchester Royal Infirmary and Regional Unit Lead for Trauma & Limb Reconstruction. He holds faculty positions on national and international training courses, contributes to peer-reviewed literature and orthopaedic textbooks, and was shortlisted for North West Deanery Orthopaedic Trainer of the Year 2025.
Conditions and procedures.
A focused practice in lower limb reconstruction, salvage and infection — drawing on circular frame surgery, hexapod fixation, intramedullary techniques and modern soft-tissue strategies.
Open & Complex Fractures
Management of high-energy lower limb trauma, including open tibial fractures, soft-tissue compromise and the early decisions that determine long-term function.
Major TraumaBone Infection & Osteomyelitis
Comprehensive treatment of acute and chronic bone infection, fracture-related infection, and the staged reconstruction of infected non-unions.
ReconstructionMal-union & Non-union
Correction of failed fracture healing using circular frames, hexapod systems and intramedullary devices — restoring alignment, length and function.
Salvage SurgeryLimb Length & Deformity
Multiplanar deformity correction and limb lengthening for both congenital and post-traumatic length discrepancy and angular or rotational deformity.
ReconstructionPeri-articular Fractures
Specialist management of fractures around the knee and ankle, including complex tibial plateau and pilon injuries with associated soft-tissue injury.
Major TraumaCompartment Syndrome
Acute decompression and the long-term management of compartment syndrome and its sequelae, including reconstruction of the post-compartment limb.
Acute CareTransverse Cortical Tibial Transport.
A regenerative surgical technique that promotes neovascularisation in the lower limb. One of very few centres in Europe offering this, and the only UK centre using TTT to treat vascular ulceration and claudication pain.
TTT is a microsurgical bone-transport technique pioneered for the salvage of limbs threatened by ischaemic ulceration, diabetic foot complications and the chronic pain of severe peripheral arterial disease. By gradually transporting a small window of cortical bone, the procedure stimulates the formation of new microvasculature in the affected limb.
At Manchester, the service is delivered by a dedicated multi-disciplinary team alongside vascular surgery, allowing patients with limb-threatening disease to be assessed, treated and supported through a structured pathway that few centres in the world can offer.
Refer a patient →From first contact to ongoing care.
Patients reach Mr Nesbitt’s practice through three principal routes. Early discussion is always welcome — particularly for complex or limb-threatening problems where time matters.
NHS Tertiary Referral
For complex trauma, infection, deformity and TTT, refer via the Manchester Limb Reconstruction Unit at Manchester Royal Infirmary. Direct discussion with Mr Nesbitt is encouraged for time-critical cases.
Private & Self-Pay
Private consultations at Etherow Health, Glossop. Patients may self-refer or be referred by their GP or consultant. Recognised by major UK insurers.
Medico-Legal
Expert witness instructions accepted via Pathway Expert Chambers, covering polytrauma, open fractures, compartment syndrome, fracture-related infection and mal/non-union — claimant or defendant. Read more →
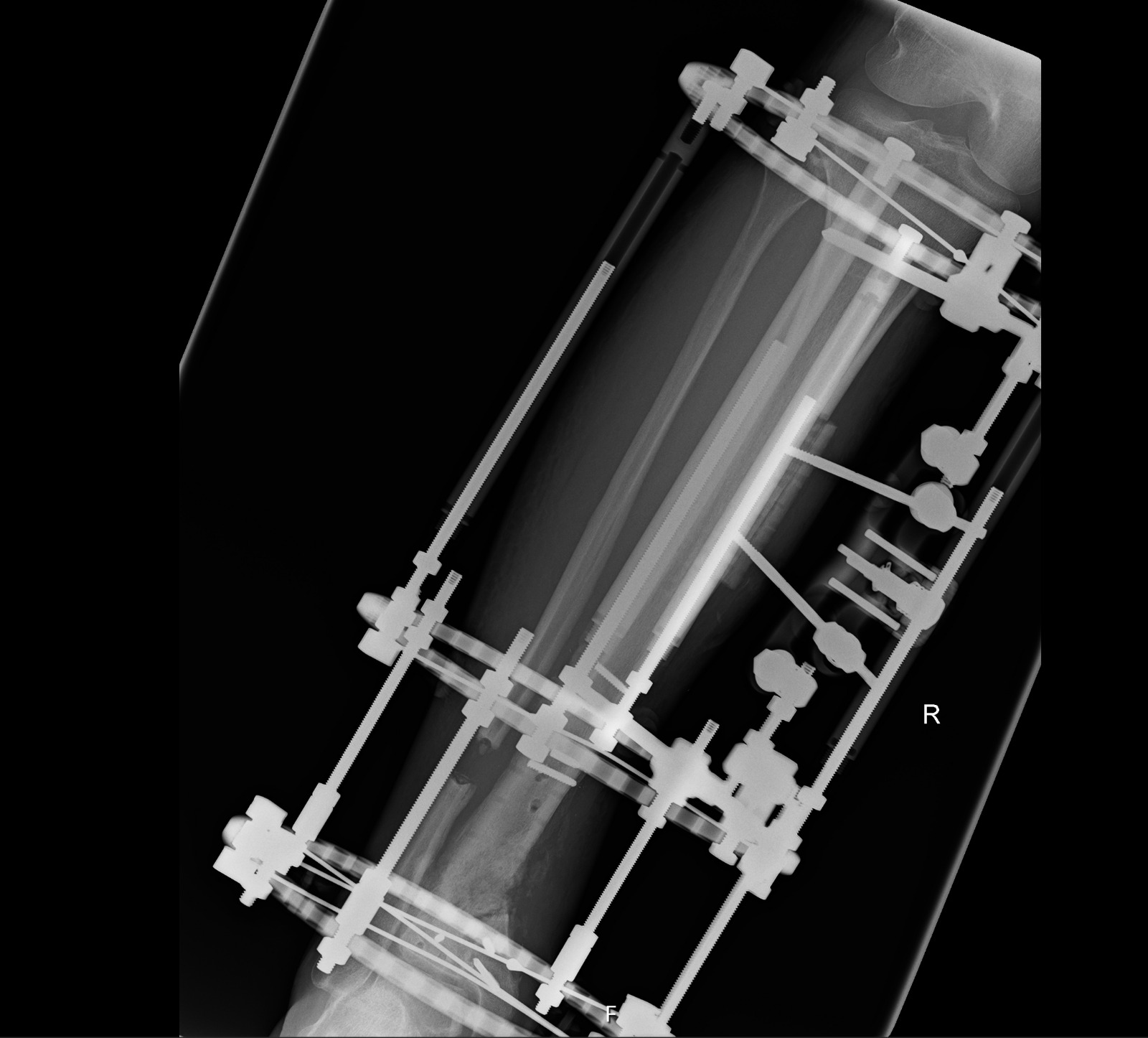
Living with a frame.
Practical, surgeon-led guidance for patients undergoing treatment with a circular frame. The summary below is drawn from the full patient booklet, which is available to download and which your specialist nurse will go through with you in person.
A surgeon-authored booklet covering the full treatment journey — types of frame, preparing for surgery, pin-site care, common problems, follow-up, frame removal and the practical questions of daily life. Sixteen pages.
Download the booklet ↓Wearing a circular frame is unfamiliar to most patients and the first weeks can feel daunting. With a settled routine, good pin-site hygiene and clear lines of contact with the clinical team, most people adapt quickly and continue with much of their day-to-day life. On average, a frame is on for about four and a half months from fitting to removal, though this varies with the injury, your general health, and how well your bone heals.
Pin-site care at home.
Pin-site care is the single most important thing you will do at home. Clean your pin sites once a week using chlorhexidine (the pink solution), and change all of the dressings at the same time. The full routine is set out below.
- Once a week — clean the pin sites and change every dressing. Between cleans, the limb is kept completely dry.
- Shower with the frame — you can shower the leg and frame once a week, immediately after cleaning the pins.
- Use chlorhexidine — the pink solution provided by the clinic. Do not use other antiseptics, ointments or creams on the pin sites.
- Leave crusts in place — do not pick or remove the crusts that form around the pins. They are part of normal healing.
- Keep the limb dry — for the rest of the week, the pin sites and frame should be kept completely dry.
- Your specialist nurse will guide you — the routine is demonstrated in person before discharge, and the video below walks through it step by step.
The video below was made by our specialist nurse, Rex Turita, and demonstrates the weekly routine step by step. We recommend watching it before your first independent pin-site care at home, and as often as you find helpful afterwards.
Helping your body to heal.
A few simple things make a real difference to how quickly your bone heals and how long you spend in the frame. These are covered in detail in the booklet, but in brief:
- Stop smoking and vaping — the single most important thing you can do. Smoking roughly doubles the time you spend in the frame, to around nine months on average, and increases the risk of pin-site infection and slow wound healing.
- Avoid alcohol — alcohol reduces calcium absorption and slows bone healing. Try to avoid it completely throughout treatment.
- Avoid anti-inflammatory medicines — drugs like ibuprofen and diclofenac slow bone healing. Paracetamol is fine, and we will prescribe stronger painkillers if needed.
- Eat well — a balanced diet rich in calcium, vitamin C and vitamin D supports healing. Short periods of sunlight in summer help vitamin D naturally.
Recognising a pin-site infection.
Around half of patients in a circular frame will develop a pin-site infection at some point. This is common and usually quickly resolved if we hear about it early. Please do not go to your GP. Instead, send a photograph and a message to our specialist team at Manchester Royal Infirmary, who can review and arrange treatment promptly.
Contact the specialist team if you notice any of the following:
- Increased pain around a pin site.
- Redness, swelling, or warmth at a pin site.
- Oozing — either bleeding, or yellow and cloudy discharge.
- Feeling generally unwell, with a fever.
Follow-up and frame removal.
After surgery, you will be seen in the frame clinic at two weeks, then at six weeks, then every six weeks until the frame comes off. During active turns or adjustments, we see you every one to two weeks to check your progress. Your specialist nurse will give you a direct contact number for any questions or concerns between visits.
Before removal, you will go through a period of dynamization, where parts of the frame are gradually loosened to confirm the bone has fully healed. Once we are satisfied, the frame is taken off in the clinic procedure room using inhaled gas-and-air for pain relief. Almost all frames come off this way. Occasionally, if a patient feels very anxious, we will remove the frame in theatre instead.
A boot or cast may be needed for a short period afterwards while things settle. The pin sites must remain dry until they have healed before you can return to daily showering.
If something doesn’t feel right.
Your treatment is a journey, and there may be bumps along the way. You will be given a direct telephone number for the specialist team while your frame is on, and you can call this number whenever you are worried about something.
If possible, please ring the clinic before attending an accident and emergency department. We can usually advise on the best place to be seen, which is not always the nearest A&E. Earlier contact is almost always better than later, and we would always rather hear from you than have you wait at home, uncertain.
Make an enquiry.
For clinical enquiries, please email directly. For medico-legal instructions, please contact Pathway Expert Chambers.
Patients, GPs & Consultants
Direct email enquiries are answered personally. Please include relevant clinical details, imaging reports and your contact information so that Mr Nesbitt can advise on the most appropriate next step.
- Emailpnesbitt@themanchesterframesurgeon.com
- NHSManchester Foundation Trust
- PrivateEtherow Health, Glossop
- LinkedInlinkedin.com/in/paul-nesbitt
Expert Witness Instructions
Mr Nesbitt accepts instructions in trauma and limb reconstruction matters through Pathway Expert Chambers. Areas of expertise include polytrauma, open fractures, compartment syndrome, fracture-related infection and mal/non-union.
- ChambersPathway Expert Chambers
- Emailinfo@pathwaychambers.com
- PracticeClaimant & Defendant